Version en español
Version en español
MATERIAL AND METHODS
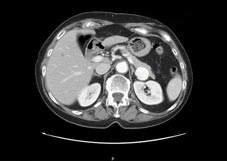
Material & Methods. The dimensions of the SAAs were between 2,5 and 3 cm, which were incidentally found during the abdominal CT scan (Photo n. 1).
|
|
|
Photo 1. CT scan image with 3D reconstructions.
|
|
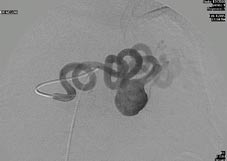
Photo 2. Angiography image.
|
Neither of the 2 SAAs were treatable with an endovascular approach because ofthe tortuousness of the proximal splenic artery (Photo n. 2).
Procedure description: the patients were placed in a 45-degree right semidecubitus (right-side down) position. Four trocars were used in both cases, one 12-mm trocar and a combination of 5 and 10-mm trocars. A 10-mm, 30-degree laparoscope was used (Photo n. 3).
|
|
|
Photo 3 . Trocars position.
|
|
|
In both patients, the gastrocolic ligament was opened using Ultracision, thereby accessing the lesser space. The splenic artery was subsequentely visualized. To get a larger view of the splenic artery, the stomach was pulled up. The splenic artery was subsequentely dissected proximally and distally to the aneurysm necks. Aneurysm exclusion was realized by laparoscopic clips on each end. The aneurysm was then totally dissected to look for a collateral arterial branch and removed in an impermeable nylon bag (Photo n. 4).
Subsequentely the proximal and distal splenic artery was prepared for the anastomosis. Anastomosis was performed with the aid of the robot da Vinci (Photo n. 5). A drain was placed next to the anastomosis.
|
Photo 5 . Robot position.
|